This website uses cookies to ensure you get the best experience on our website.
- Table of Contents
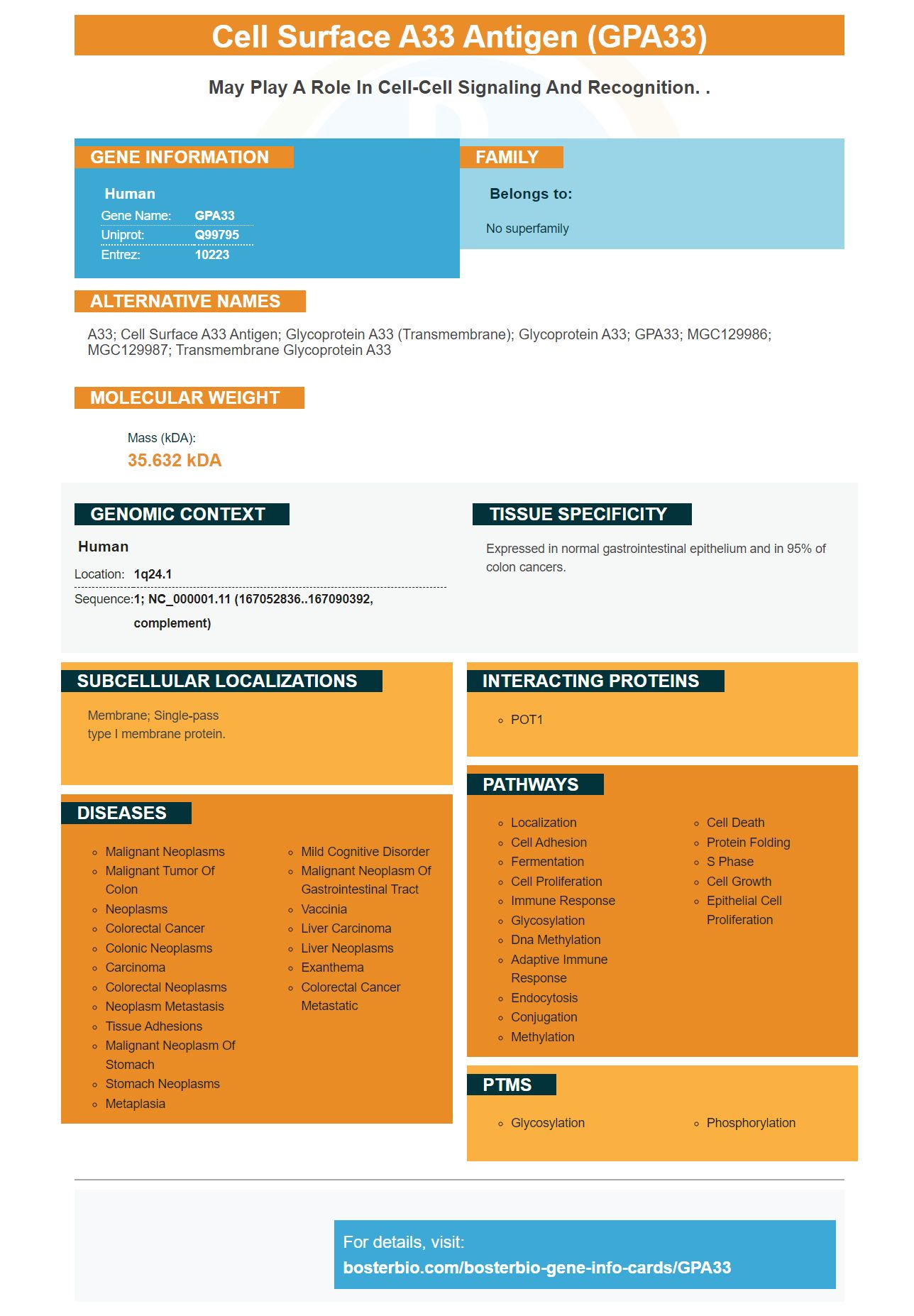
Facts about Cell surface A33 antigen.

| Human | |
|---|---|
| Gene Name: | GPA33 |
| Uniprot: | Q99795 |
| Entrez: | 10223 |

| Belongs to: |
|---|
| No superfamily |

A33; cell surface A33 antigen; glycoprotein A33 (transmembrane); Glycoprotein A33; GPA33; MGC129986; MGC129987; transmembrane glycoprotein A33
Mass (kDA):
35.632 kDA

| Human | |
|---|---|
| Location: | 1q24.1 |
| Sequence: | 1; NC_000001.11 (167052836..167090392, complement) |
Expressed in normal gastrointestinal epithelium and in 95% of colon cancers.
Membrane; Single-pass type I membrane protein.




PMID: 9012807 by Heath J.K., et al. The human A33 antigen is a transmembrane glycoprotein and a novel member of the immunoglobulin superfamily.
PMID: 9245713 by Ritter G., et al. Characterization of posttranslational modifications of human A33 antigen, a novel palmitoylated surface glycoprotein of human gastrointestinal epithelium.


