This website uses cookies to ensure you get the best experience on our website.
- Table of Contents
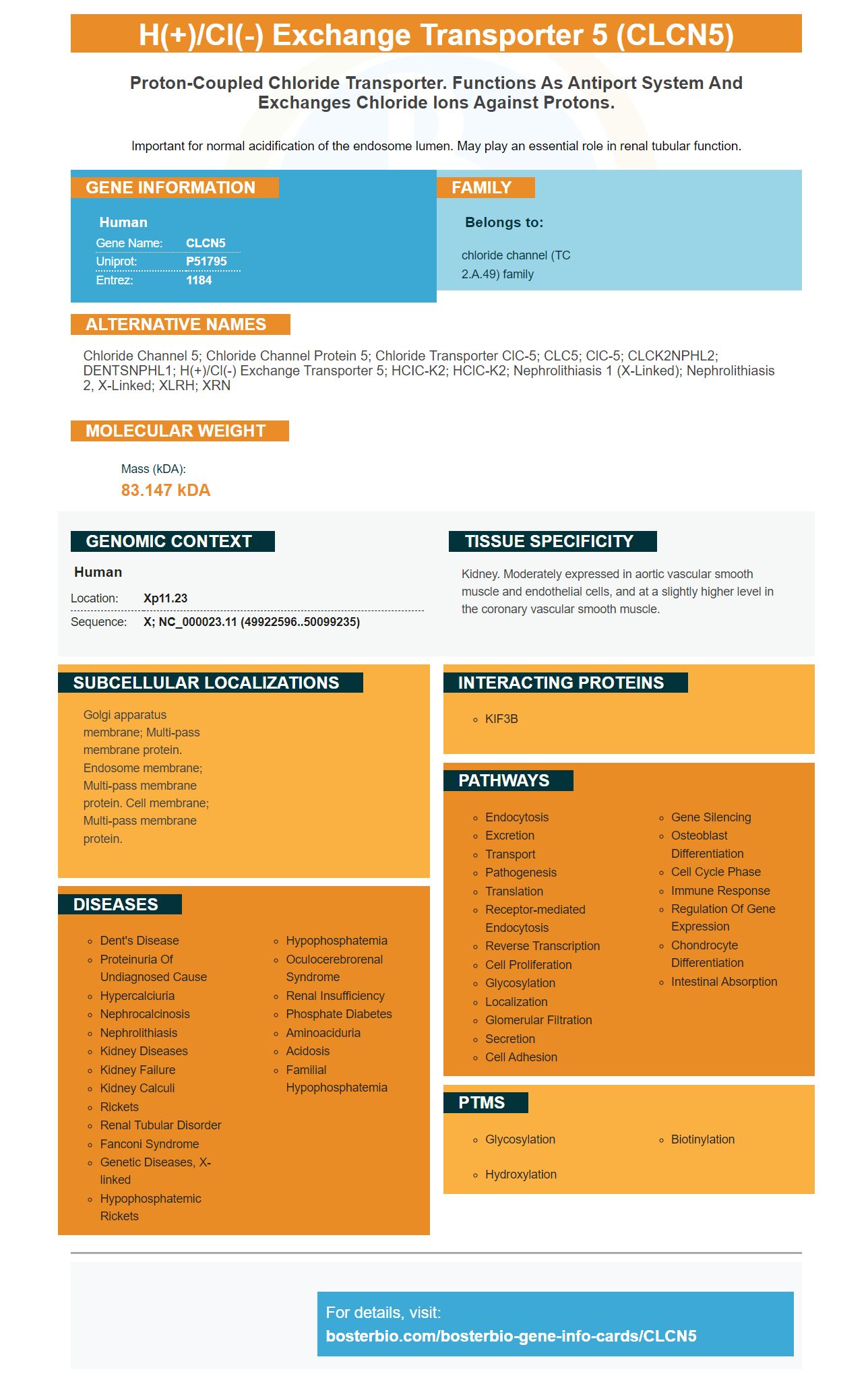
Facts about H(+)/Cl(-) exchange transporter 5.

Important for normal acidification of the endosome lumen. May play an essential role in renal tubular function.
| Human | |
|---|---|
| Gene Name: | CLCN5 |
| Uniprot: | P51795 |
| Entrez: | 1184 |

| Belongs to: |
|---|
| chloride channel (TC 2.A.49) family |

chloride channel 5; Chloride channel protein 5; Chloride transporter ClC-5; CLC5; clC-5; CLCK2NPHL2; DENTSNPHL1; H(+)/Cl(-) exchange transporter 5; hCIC-K2; hClC-K2; nephrolithiasis 1 (X-linked); nephrolithiasis 2, X-linked; XLRH; XRN
Mass (kDA):
83.147 kDA

| Human | |
|---|---|
| Location: | Xp11.23 |
| Sequence: | X; NC_000023.11 (49922596..50099235) |
Kidney. Moderately expressed in aortic vascular smooth muscle and endothelial cells, and at a slightly higher level in the coronary vascular smooth muscle.
Golgi apparatus membrane; Multi-pass membrane protein. Endosome membrane; Multi-pass membrane protein. Cell membrane; Multi-pass membrane protein.




PMID: 8575751 by Fisher S.E., et al. Cloning and characterization of CLCN5, the human kidney chloride channel gene implicated in Dent disease (an X-linked hereditary nephrolithiasis).
PMID: 7874126 by Fisher S., et al. Isolation and partial characterization of a chloride channel gene which is expressed in kidney and is a candidate for Dent's disease (an X-linked hereditary nephrolithiasis).


