This website uses cookies to ensure you get the best experience on our website.
- Table of Contents

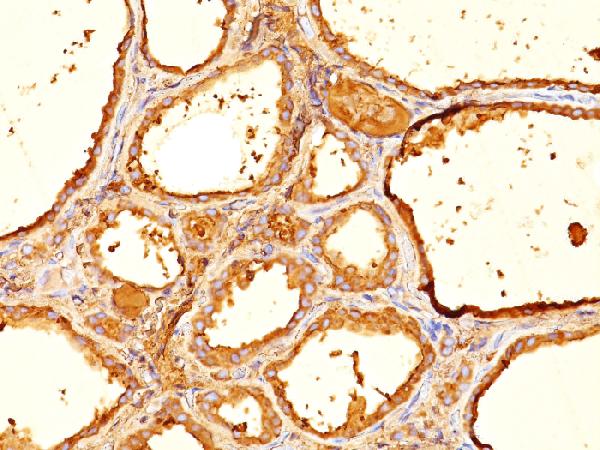


Facts about Thyroglobulin.
| Human | |
|---|---|
| Gene Name: | TG |
| Uniprot: | P01266 |
| Entrez: | 7038 |

| Belongs to: |
|---|
| type-B carboxylesterase/lipase family |

AITD3; AITD3TGN; cog; TDH3; Tg; TGN; Thyroglobulin
Mass (kDA):
304.79 kDA

| Human | |
|---|---|
| Location: | 8q24.22 |
| Sequence: | 8; NC_000008.11 (132866943..133134902) |
Thyroid gland specific.
Secreted. Secreted into the thyroid follicle lumen (PubMed:19509106). Localizes to colloid globules, a structure formed in the thyroid follicle lumen consisting of cross-linked TG arranged in concentric layers (PubMed:8626858, PubMed:11082042).



PMID: 3595599 by Malthiery Y., et al. Primary structure of human thyroglobulin deduced from the sequence of its 8448-base complementary DNA.
PMID: 9186272 by van de Graaf S.A.R., et al. The revised 8307 base pair coding sequence of human thyroglobulin transiently expressed in eukaryotic cells.