This website uses cookies to ensure you get the best experience on our website.
- Table of Contents
2 Citations 7 Q&As



Facts about Syndecan-3.

.
| Human | |
|---|---|
| Gene Name: | SDC3 |
| Uniprot: | O75056 |
| Entrez: | 9672 |

| Belongs to: |
|---|
| syndecan proteoglycan family |

KIAA0468; N-Syndecan; SDC3; SDCN; SYND3syndecan proteoglycan 3; syndecan 3 (N-syndecan); syndecan 3; syndecan neural type; Syndecan3; Syndecan-3
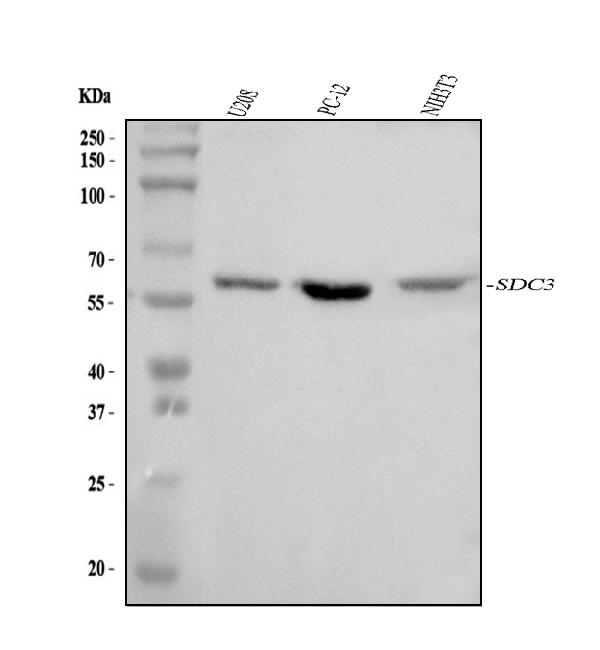
Mass (kDA):
45.497 kDA

| Human | |
|---|---|
| Location: | 1p35.2 |
| Sequence: | 1; NC_000001.11 (30869466..30909735, complement) |
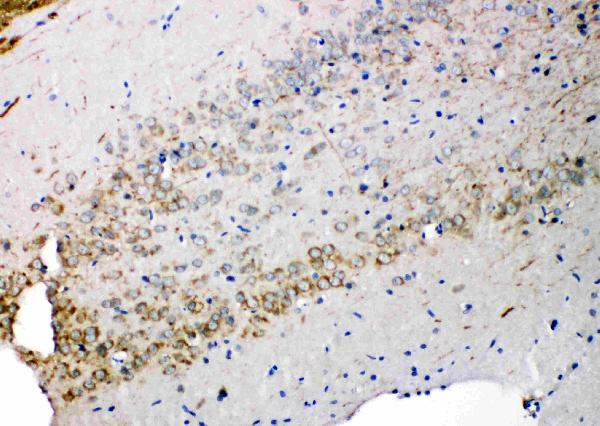
Expressed in the nervous system, the adrenal gland, and the spleen.
Cell membrane; Single-pass type I membrane protein.




PMID: 11527150 by Berndt C., et al. Cloning and characterization of human syndecan-3.
PMID: 9388509 by Asundi V.K., et al. Phosphorylation of recombinant N-syndecan (syndecan 3) core protein.
*More publications can be found for each product on its corresponding product page
