This website uses cookies to ensure you get the best experience on our website.
- Table of Contents
Facts about Pyrin.

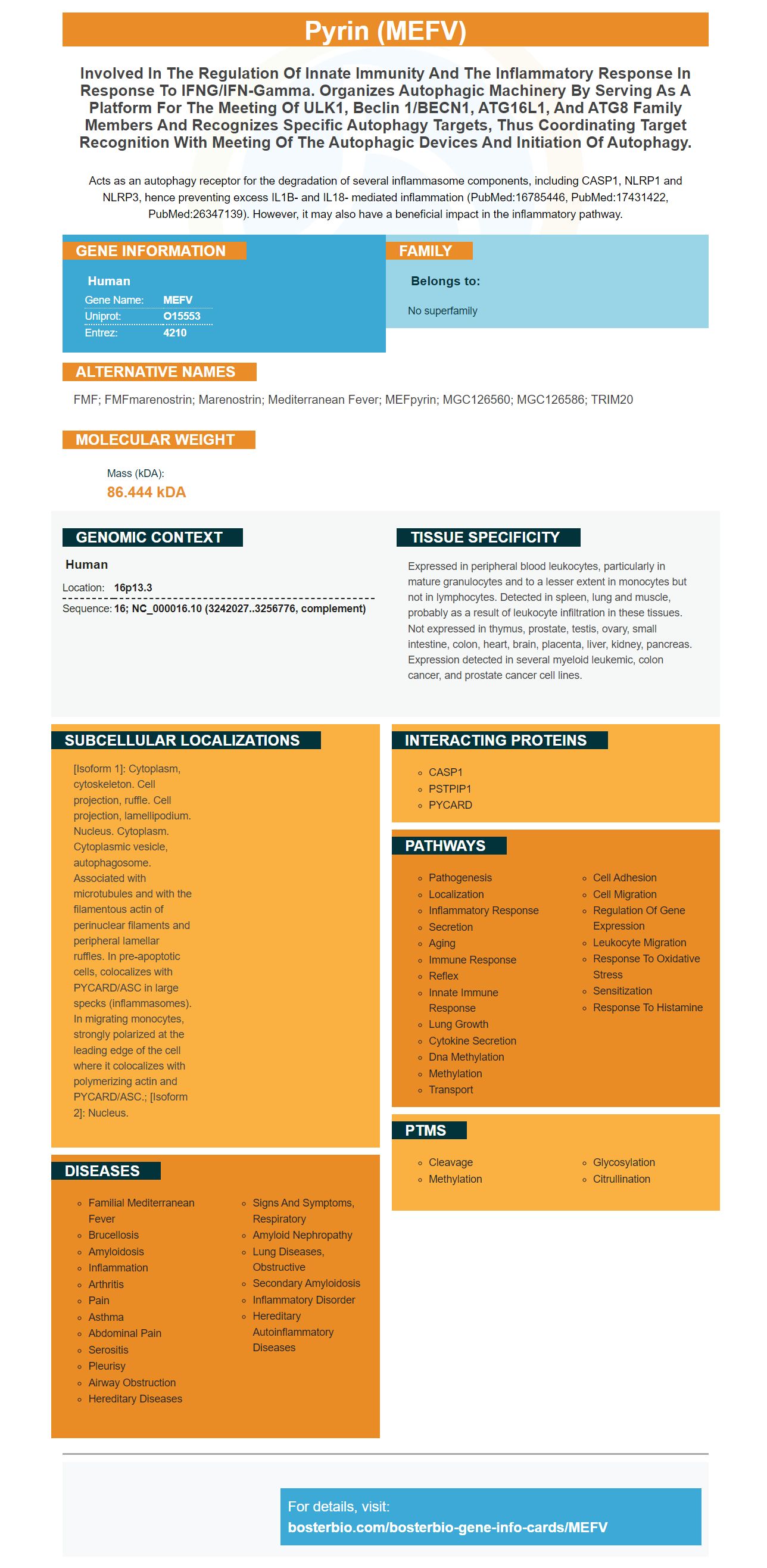
Acts as an autophagy receptor for the degradation of several inflammasome components, including CASP1, NLRP1 and NLRP3, hence preventing excess IL1B- and IL18- mediated inflammation (PubMed:16785446, PubMed:17431422, PubMed:26347139). However, it may also have a beneficial impact in the inflammatory pathway.
| Human | |
|---|---|
| Gene Name: | MEFV |
| Uniprot: | O15553 |
| Entrez: | 4210 |

| Belongs to: |
|---|
| No superfamily |

FMF; FMFmarenostrin; Marenostrin; Mediterranean fever; MEFpyrin; MGC126560; MGC126586; TRIM20
Mass (kDA):
86.444 kDA

| Human | |
|---|---|
| Location: | 16p13.3 |
| Sequence: | 16; NC_000016.10 (3242027..3256776, complement) |
Expressed in peripheral blood leukocytes, particularly in mature granulocytes and to a lesser extent in monocytes but not in lymphocytes. Detected in spleen, lung and muscle, probably as a result of leukocyte infiltration in these tissues. Not expressed in thymus, prostate, testis, ovary, small intestine, colon, heart, brain, placenta, liver, kidney, pancreas. Expression detected in several myeloid leukemic, colon cancer, and prostate cancer cell lines.
[Isoform 1]: Cytoplasm, cytoskeleton. Cell projection, ruffle. Cell projection, lamellipodium. Nucleus. Cytoplasm. Cytoplasmic vesicle, autophagosome. Associated with microtubules and with the filamentous actin of perinuclear filaments and peripheral lamellar ruffles. In pre-apoptotic cells, colocalizes with PYCARD/ASC in large specks (inflammasomes). In migrating monocytes, strongly polarized at the leading edge of the cell where it colocalizes with polymerizing actin and PYCARD/ASC.; [Isoform 2]: Nucleus.




PMID: 9288758 by Aksentijevich I., et al. Ancient missense mutations in a new member of the RoRet gene family are likely to cause familial Mediterranean fever.
PMID: 11115844 by Papin S., et al. Alternative splicing at the MEFV locus involved in familial Mediterranean fever regulates translocation of the marenostrin/pyrin protein to the nucleus.