This website uses cookies to ensure you get the best experience on our website.
- Table of Contents


Facts about C-C chemokine receptor type 9.

Receptor for chemokine SCYA25/TECK.
Subsequently transduces a signal by increasing the intracellular calcium ions level..
| Human | |
|---|---|
| Gene Name: | CCR9 |
| Uniprot: | P51686 |
| Entrez: | 10803 |

| Belongs to: |
|---|
| G-protein coupled receptor 1 family |

C-C chemokine receptor type 9; C-C CKR-9; CC-CKR-9; CCR9; CCR-9; CD199; CDw199 antigen; CDw199; chemokine (C-C motif) receptor 9; G protein-coupled receptor 28; GPR28; GPR-9-6G-protein coupled receptor 28
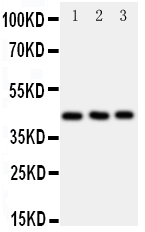
Mass (kDA):
42.016 kDA

| Human | |
|---|---|
| Location: | 3p21.31 |
| Sequence: | 3; NC_000003.12 (45886504..45903177) |
Highly expressed in the thymus and low in lymph nodes and spleen.
Cell membrane; Multi-pass membrane protein.



PMID: 10229797 by Zaballos A., et al. Identification of the orphan chemokine receptor GPR-9-6 as CCR9, the receptor for the chemokine TECK.
PMID: 10640743 by Yu C.-R., et al. CCR9A and CCR9B: two receptors for the chemokine CCL25/TECK/Ck beta- 15 that differ in their sensitivities to ligand.

