This website uses cookies to ensure you get the best experience on our website.
- Table of Contents
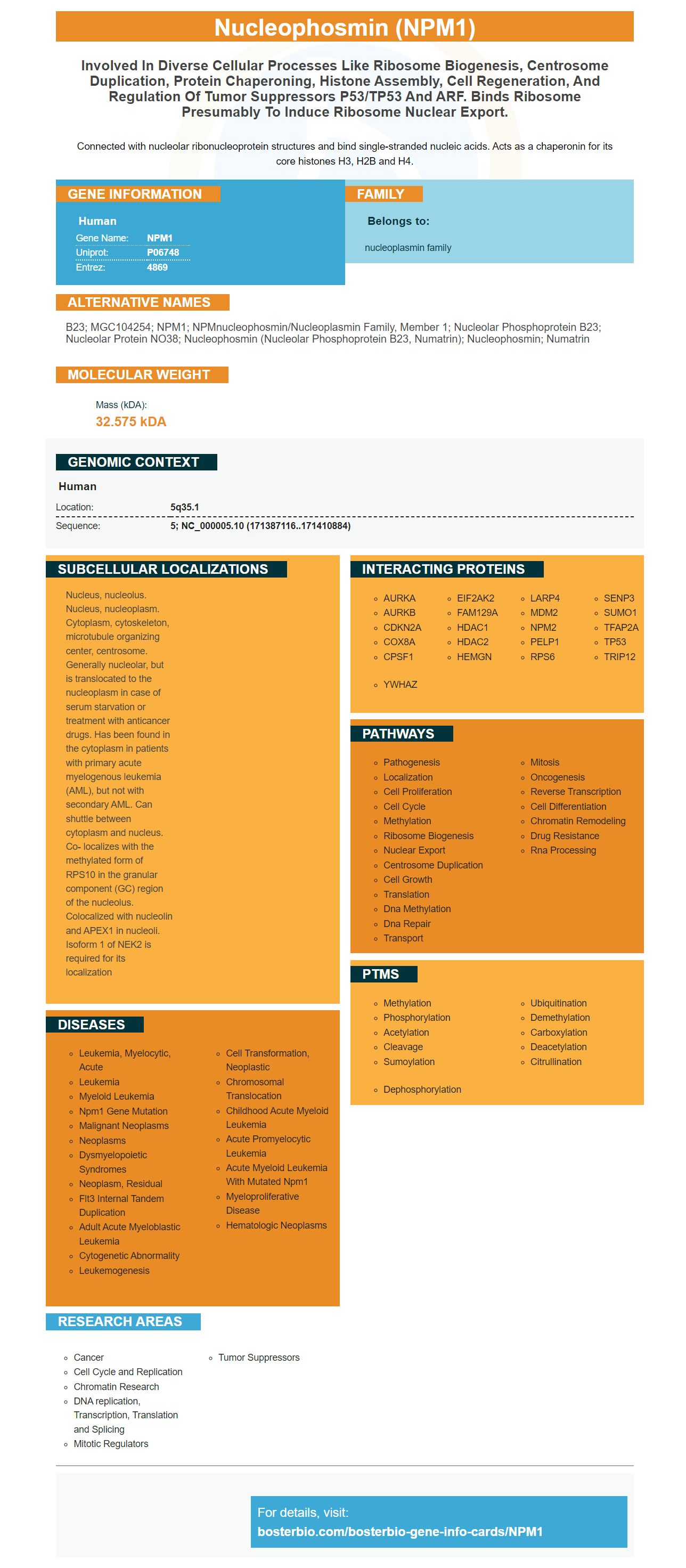










Facts about Nucleophosmin.

Connected with nucleolar ribonucleoprotein structures and bind single-stranded nucleic acids. Acts as a chaperonin for its core histones H3, H2B and H4.
| Human | |
|---|---|
| Gene Name: | NPM1 |
| Uniprot: | P06748 |
| Entrez: | 4869 |

| Belongs to: |
|---|
| nucleoplasmin family |

B23; MGC104254; NPM1; NPMnucleophosmin/nucleoplasmin family, member 1; Nucleolar phosphoprotein B23; Nucleolar protein NO38; nucleophosmin (nucleolar phosphoprotein B23, numatrin); Nucleophosmin; Numatrin
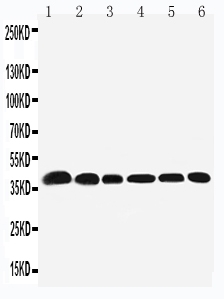
Mass (kDA):
32.575 kDA

| Human | |
|---|---|
| Location: | 5q35.1 |
| Sequence: | 5; NC_000005.10 (171387116..171410884) |
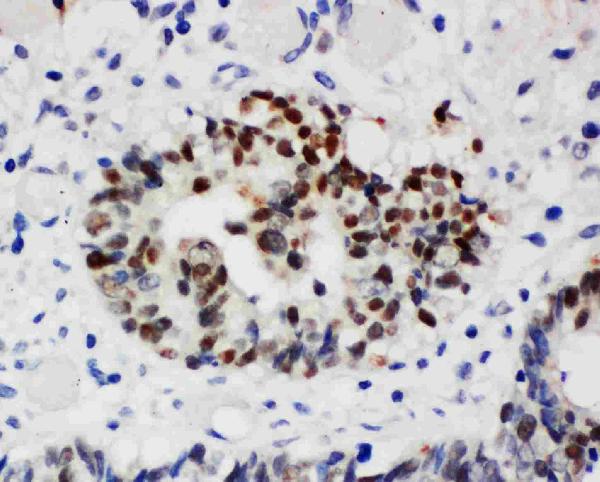
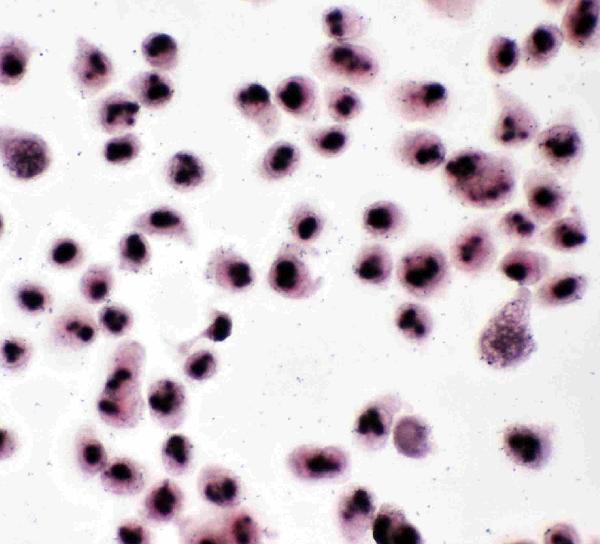
Nucleus, nucleolus. Nucleus, nucleoplasm. Cytoplasm, cytoskeleton, microtubule organizing center, centrosome. Generally nucleolar, but is translocated to the nucleoplasm in case of serum starvation or treatment with anticancer drugs. Has been found in the cytoplasm in patients with primary acute myelogenous leukemia (AML), but not with secondary AML. Can shuttle between cytoplasm and nucleus. Co- localizes with the methylated form of RPS10 in the granular component (GC) region of the nucleolus. Colocalized with nucleolin and APEX1 in nucleoli. Isoform 1 of NEK2 is required for its localization




PMID: 2713355 by Chan W.-Y., et al. Characterization of the cDNA encoding human nucleophosmin and studies of its role in normal and abnormal growth.
PMID: 2775293 by Li X., et al. The nucleotide sequence of a human cDNA encoding the highly conserved nucleolar phosphoprotein B23.