This website uses cookies to ensure you get the best experience on our website.
- Table of Contents
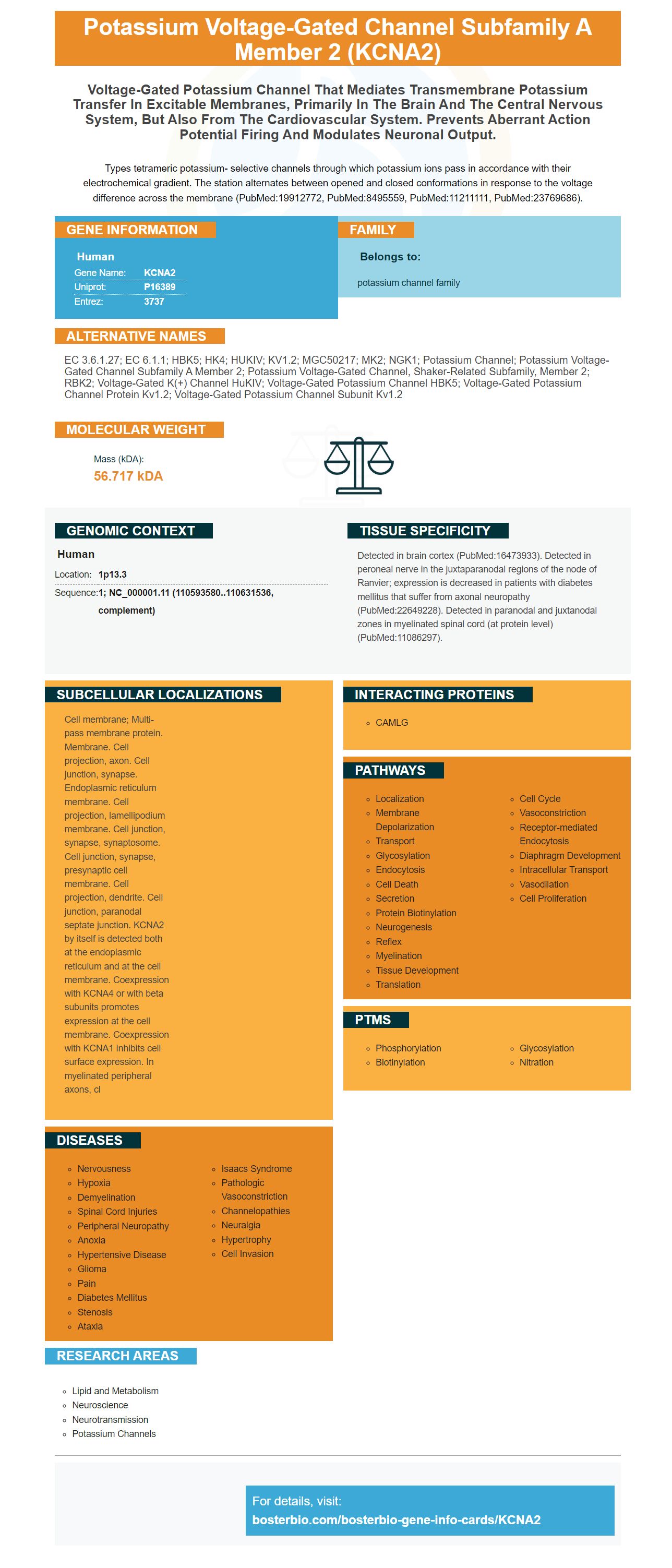
Facts about Potassium voltage-gated channel subfamily A member 2.

Types tetrameric potassium- selective channels through which potassium ions pass in accordance with their electrochemical gradient. The station alternates between opened and closed conformations in response to the voltage difference across the membrane (PubMed:19912772, PubMed:8495559, PubMed:11211111, PubMed:23769686).
| Human | |
|---|---|
| Gene Name: | KCNA2 |
| Uniprot: | P16389 |
| Entrez: | 3737 |

| Belongs to: |
|---|
| potassium channel family |

EC 3.6.1.27; EC 6.1.1; HBK5; HK4; HUKIV; KV1.2; MGC50217; MK2; NGK1; potassium channel; potassium voltage-gated channel subfamily A member 2; potassium voltage-gated channel, shaker-related subfamily, member 2; RBK2; Voltage-gated K(+) channel HuKIV; Voltage-gated potassium channel HBK5; voltage-gated potassium channel protein Kv1.2; Voltage-gated potassium channel subunit Kv1.2
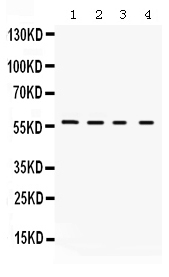
Mass (kDA):
56.717 kDA

| Human | |
|---|---|
| Location: | 1p13.3 |
| Sequence: | 1; NC_000001.11 (110593580..110631536, complement) |
Detected in brain cortex (PubMed:16473933). Detected in peroneal nerve in the juxtaparanodal regions of the node of Ranvier; expression is decreased in patients with diabetes mellitus that suffer from axonal neuropathy (PubMed:22649228). Detected in paranodal and juxtanodal zones in myelinated spinal cord (at protein level) (PubMed:11086297).
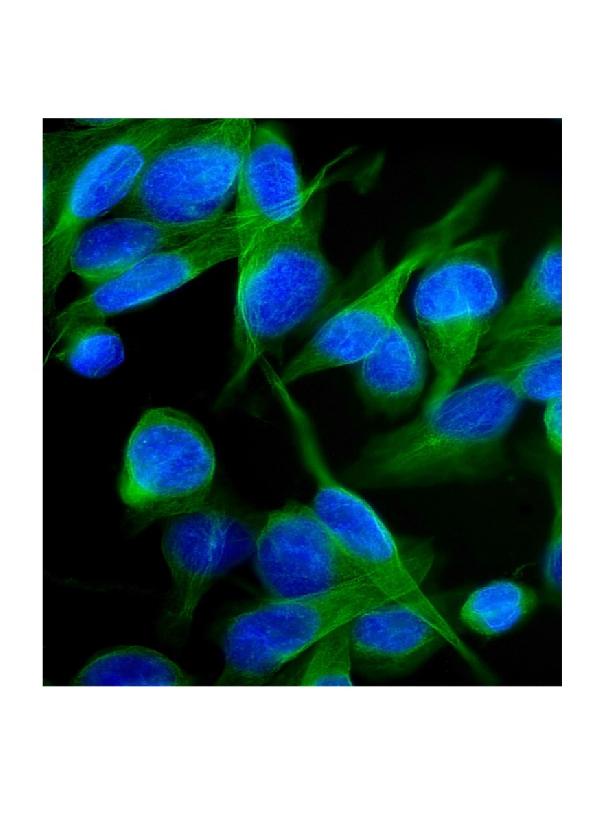
Cell membrane; Multi-pass membrane protein. Membrane. Cell projection, axon. Cell junction, synapse. Endoplasmic reticulum membrane. Cell projection, lamellipodium membrane. Cell junction, synapse, synaptosome. Cell junction, synapse, presynaptic cell membrane. Cell projection, dendrite. Cell junction, paranodal septate junction. KCNA2 by itself is detected both at the endoplasmic reticulum and at the cell membrane. Coexpression with KCNA4 or with beta subunits promotes expression at the cell membrane. Coexpression with KCNA1 inhibits cell surface expression. In myelinated peripheral axons, cl




PMID: 19912772 by Ramaswami M., et al. Human potassium channel genes: molecular cloning and functional expression.
PMID: 8495559 by Po S., et al. Heteromultimeric assembly of human potassium channels. Molecular basis of a transient outward current?