This website uses cookies to ensure you get the best experience on our website.
- Table of Contents
Facts about Hepatocyte nuclear factor 3-alpha.

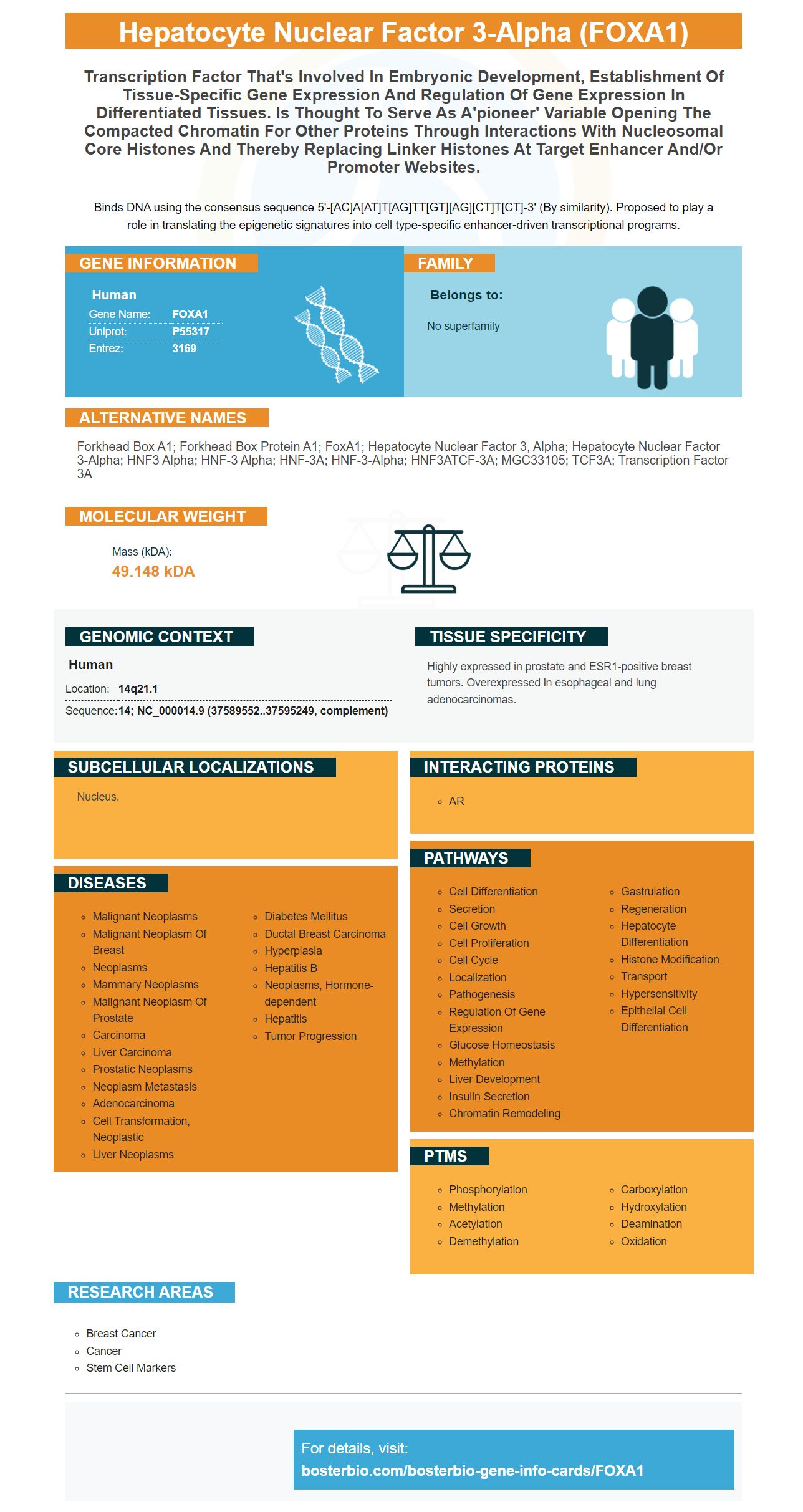
Binds DNA using the consensus sequence 5'-[AC]A[AT]T[AG]TT[GT][AG][CT]T[CT]-3' (By similarity). Proposed to play a role in translating the epigenetic signatures into cell type-specific enhancer-driven transcriptional programs.
| Human | |
|---|---|
| Gene Name: | FOXA1 |
| Uniprot: | P55317 |
| Entrez: | 3169 |

| Belongs to: |
|---|
| No superfamily |

forkhead box A1; Forkhead box protein A1; FoxA1; hepatocyte nuclear factor 3, alpha; hepatocyte nuclear factor 3-alpha; HNF3 alpha; HNF-3 alpha; HNF-3A; HNF-3-alpha; HNF3ATCF-3A; MGC33105; TCF3A; Transcription factor 3A
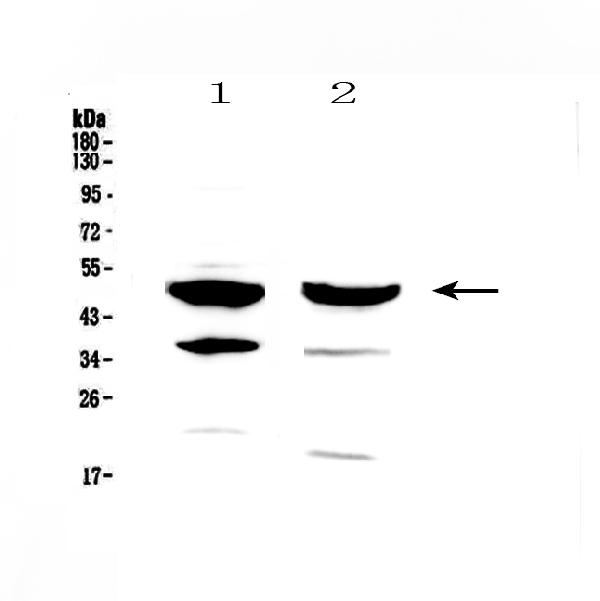
Mass (kDA):
49.148 kDA

| Human | |
|---|---|
| Location: | 14q21.1 |
| Sequence: | 14; NC_000014.9 (37589552..37595249, complement) |
Highly expressed in prostate and ESR1-positive breast tumors. Overexpressed in esophageal and lung adenocarcinomas.
Nucleus.




PMID: 8652662 by Bingle C.D., et al. Molecular cloning of the forkhead transcription factor HNF-3 alpha from a human pulmonary adenocarcinoma cell line.
PMID: 10899756 by Navas M.A., et al. The human HNF-3 genes: cloning, partial sequence and mutation screening in patients with impaired glucose homeostasis.