This website uses cookies to ensure you get the best experience on our website.
- Table of Contents



16 Q&As



Facts about C-C chemokine receptor type 3.

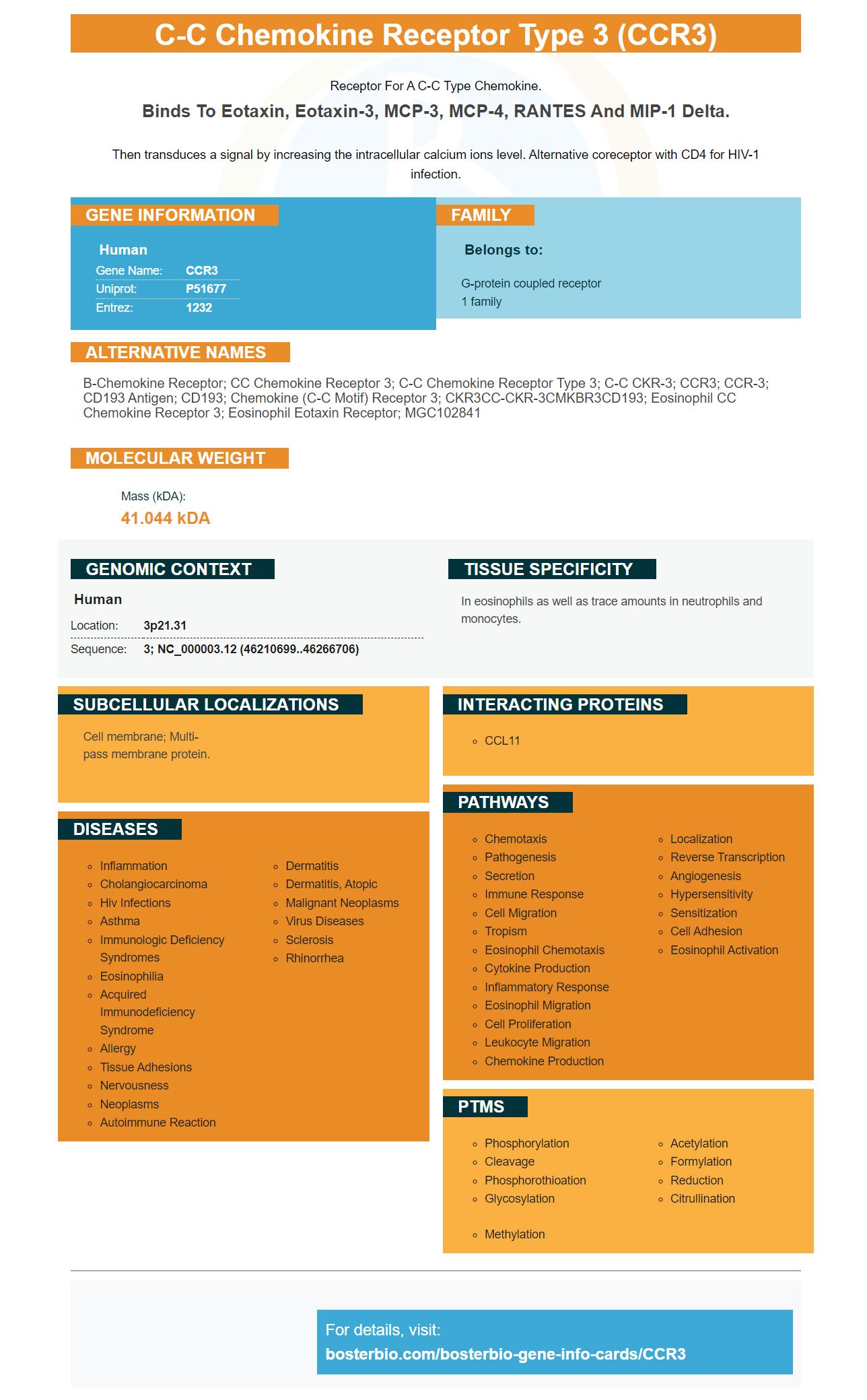
Receptor for a C-C type chemokine.
Binds to eotaxin, eotaxin-3, MCP-3, MCP-4, RANTES and MIP-1 delta.Then transduces a signal by increasing the intracellular calcium ions level. Alternative coreceptor with CD4 for HIV-1 infection.
| Human | |
|---|---|
| Gene Name: | CCR3 |
| Uniprot: | P51677 |
| Entrez: | 1232 |

| Belongs to: |
|---|
| G-protein coupled receptor 1 family |

b-chemokine receptor; CC chemokine receptor 3; C-C chemokine receptor type 3; C-C CKR-3; CCR3; CCR-3; CD193 antigen; CD193; chemokine (C-C motif) receptor 3; CKR3CC-CKR-3CMKBR3CD193; eosinophil CC chemokine receptor 3; Eosinophil eotaxin receptor; MGC102841
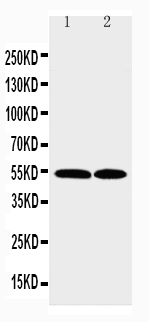
Mass (kDA):
41.044 kDA

| Human | |
|---|---|
| Location: | 3p21.31 |
| Sequence: | 3; NC_000003.12 (46210699..46266706) |
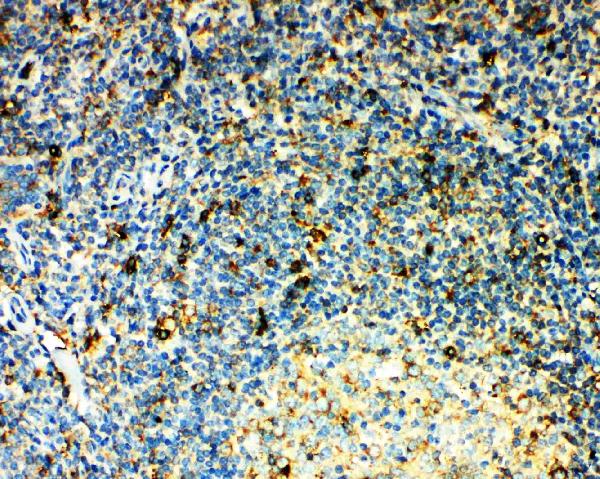
In eosinophils as well as trace amounts in neutrophils and monocytes.
Cell membrane; Multi-pass membrane protein.




PMID: 7622448 by Combadiere C., et al. Cloning and functional expression of a human eosinophil CC chemokine receptor.
PMID: 8642344 by Daugherty B.L., et al. Cloning, expression, and characterization of the human eosinophil eotaxin receptor.